Complete denture repair is a more difficult repair method for oral prosthesis. There are many clinical problems, which affect the repair effect. Improper treatment can even lead to repair failure, and cause damage to the oral tissue structure and physiological function in serious cases.
01
Keto break and snap repairs
1. cause
1. Cause of the patient
External force breaks, the resultant force is too large;
2. Unbalanced resultant force
Improper position of tooth arrangement;
Unbalance of anterior extension side: alveolar ridge resorption; fabrication problems; biomechanical factors
2. Stress analysis of maxillary photostock breaks
The maxillary fracture area is mostly located in the palatal rapa and the premolar area, so the anterior tooth area and the premolar area should be strengthened to improve the tensile resistance of the ginto. The lateral tensile stress in the ginto is the most important destructive stress, and the maximum tensile stress in the ginto appears in the palatal surface of the maxilla.(Photoelastic method, electrical measurement method)
During the median loading, the stress is mainly concentrated in the area between the fangs and the second premolar; during the anterior extension loading, the stress is mainly concentrated in the anterior tooth area;
During lateral loading, the stress is mainly concentrated in the area between the fangs and the first molar.(3 D light elastic method)
3. Stress analysis of mandibular stock break
The mandibular fracture area is mostly located in the anterior tooth area. The tensile stress in the middle and middle is the most important destructive stress, and the maximum tensile stress in the gbase appears in the anterior tooth area.(Photoelastic method, electric measurement method) in the middle, forward extension, lateral movement, the anterior tooth area is the stress concentration area.
Four, repair method
1, lip, buccal base broken repair
With 502 stick- - -fill gypsum model- - -remove the fracture on both sides of the base part- - - -self-coagulation plastic repair such as broken lip base lost or broken, with wax or impression paste in the base broken place, oral restore the base shape- - - - -irrigation model- - - - -box- - - - -in the model with self-coagulation plastic or hot coagulation plastic repair.
2. Repair of upper denture
Adhesive- -cast cast model- -self-coagulation plastic repair or thermal coagulation plastic repair
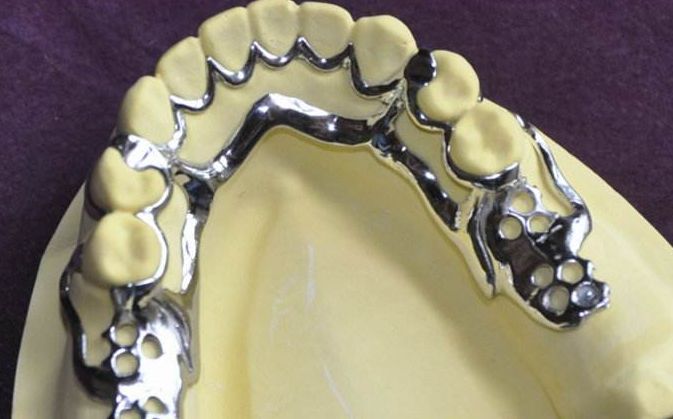
Add metal wire or metal mesh to the weak part or stress concentration part of the base to increase the strength.
picture
02Break or loss of artificial teeth
Break or loss of artificial teeth is more common in the anterior teeth.
I. The reasons
1, external force break;
2. Inclusal imbalance;
3, denture production problems, artificial teeth and base combination is not good;
2. Repair method
1. Remove the broken artificial teeth and their lingual base base;
2, choose the appropriate artificial teeth arranged on the dental arch;
3, the wax will fix it;
4. Conventional heat treatment or self-coagulation plastic;
5. Tuning;
03Full denture lining
Add a layer of plastic to the tissue surface of the complete denture base to fill the unpacked gaps.
act on
1. Restoration of the close fit of the base tissue surface with the mucosal tissue of the supporting area
2. Increase the retention force of the denture
3. It is conducive to the reasonable distribution of chewing pressure on the supporting tissue.
compliant
1. Poor retention of the denture
2, due to the warping movement caused by the base fracture
3. Pain and excessive absorption of alveolar ridge caused by uneven stress of supporting tissue
1. Direct relining
Using self-coagulation resin directly in the patient mouth, the wrong statement about direct relining:
A Direct relining is A common method of relining;
B evenly wear the tissue surface evenly 1mm;
C The self-condensing plastic used is easy to absorb heat;
D The self-coagulable plastic used easily leads to allergic reactions;
E When relining, the condensing plastic can be completely hardened before being removed;
2. Indirect lining
The denture is used as an individual tray, the final impression material is added to the tissue surface, the closed seal mold is taken, the denture and the impression material are directly boxed, and the impression material on the tissue surface is replaced with hot condensing resin.
Three, the soft lining
Line with the base tissue surface, increase the retention, buffer the chewing pressure of the mucosa in the support area, reduce the stress of the supporting tissue, avoid tenderness, and improve the mastication efficiency.
Adaptation: alveolar ridge is low flat or blade shape, thin mucous membrane, poor support ability.
Existing soft lining material denture soft lining material is used in the mouth for a long time, and contact with the oral mucosa, therefore, there are certain requirements for it.
The ideal denture soft lining material shall meet the following basic requirements:
① Good biological safety, non-toxic, non-stimulating;
② Stable chemical performance, anti-aging;
③ After curing (vulcanization) has good elasticity, and can maintain this elasticity in long-term use;
④ Can form a good combination with the base base;
⑤ In the long-term use of the oral environment is not easy to adhere to and breed bacteria, especially mold;
⑥ Water absorption rate and dissolution rate are small;
⑦ Good mechanical properties and wear resistance;
⑧ Clinical is easy to implement, easy to pad, polishing.
Unfortunately, so far, there is no soft lining material that can fully meet the above requirements.
Now there are many soft lining material products available in the domestic and foreign markets. From the perspective of its material composition, there are mainly plasticized acrylic ester soft plastics and silicone rubber. The former is mainly used for short-term soft lining, while the latter is mainly used for medium and long-term soft lining.




 Open wechat
Open wechat





 | 粤ICP备2021067230号
| 粤ICP备2021067230号